
Alex Phillips: Perilous position of the NHS exposed by pandemic


By Alex Phillips
Published: 12/08/2021
- 16:16Updated: 14/02/2023
- 11:11


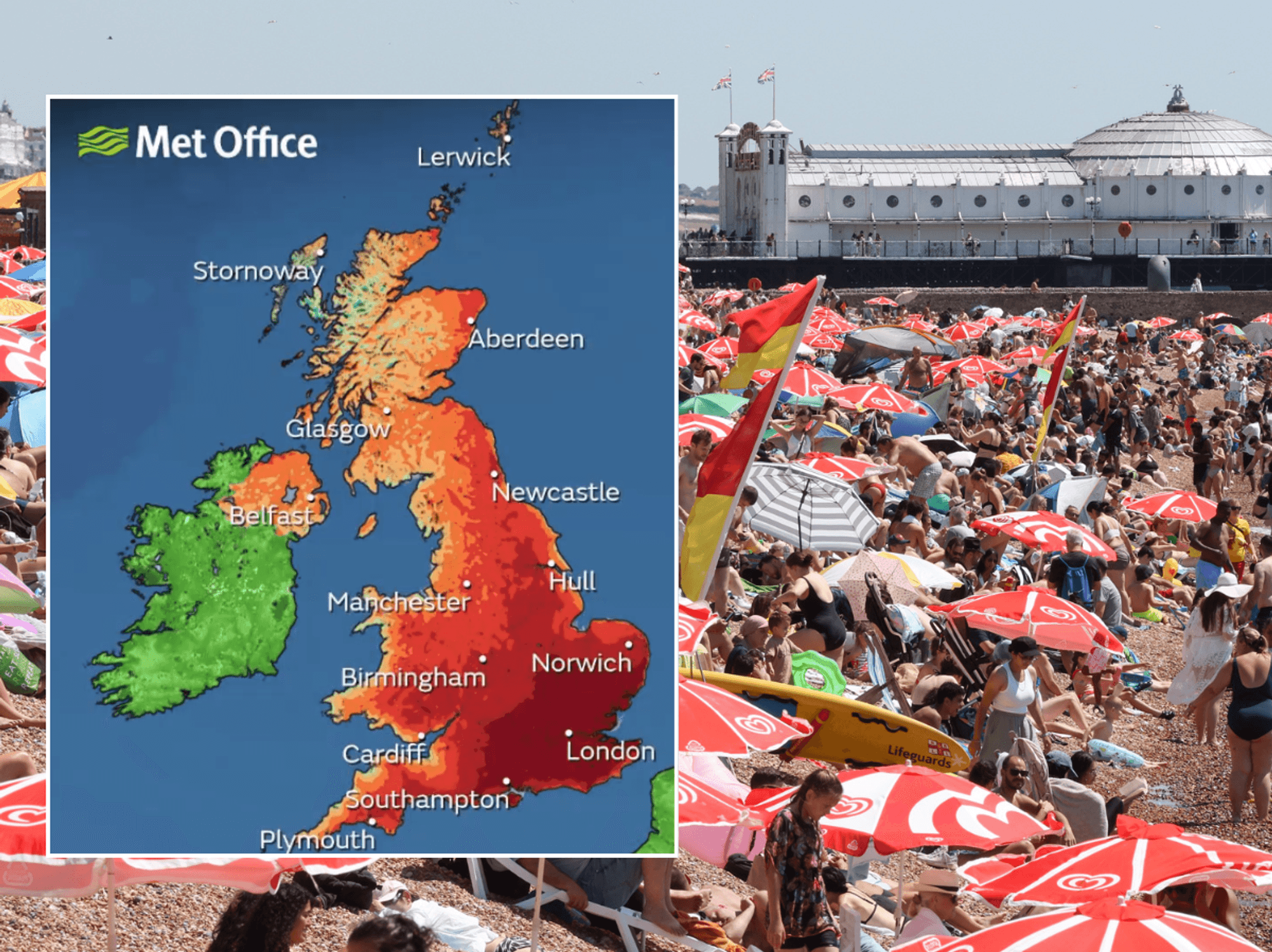
'Glance at other healthcare systems, and you find far more nuance'
Don't Miss

Most Read



Born in post war Britain to serve a population of 49 million, it’s now one of the planet’s biggest public health services, cited the world over as a paradigm of Universal Care. Come its centenary, our population could be twice the size and much older, riddled with modern chronic disorders, yet with a panoply of new drugs and innovative techniques on offer, all with their own price tag.
Being one of very few, fully free, nationalised healthcare systems in the world, it is both a national treasure and worldwide wonder. Yet some argue it is dangerously bordering on a state religion, impervious to its failings with agnostics and critics tried as heretics and blasphemers.
Yet while politicians confidently state the NHS is the envy of the world, some parts of the world look upon things rather differently. As debate raged over Obamacare the NHS was held up by some as a preventable disaster. Covid predictions on the continent cited the UK as the greatest risk due to a healthcare system that labours to be fleet of foot, and has half the ratio of beds and doctors to patients as most other European countries.
There is of course so much to be proud of. Free at the point of access and free of the horrifically dehumanising bureaucracy of bartering for treatment in the middle of a health emergency.
But pride can be anathema to progress. And the pandemic has perhaps revealed that the model dreamt up in the last century may require critical care in its elderly years.
Yet today, crucial discourse about the largest state run body, the arbiters of life and death, is silenced by a cult-like subservience to its existential nature. Anyone who dares mention the P word, privatisation, let alone the i word, insurance, must commit to incantations of ‘hard working doctors and nurses’ while clapping on the doorstep as an act of penance.
But how can a fully state-backed, chronically under-resourced service get the cash it needs? There are three choices: First, increase taxes, which is politically unpalatable. Second, nick money from other Government departments when the NHS already consumes one fifth of the entire national budget. The third option is the one nobody dares utter. Profits.
All too often a dangerously disingenuous dichotomy is presented by those who dominate the debate. The status quo, or an American model where ruthless capitalists let the poor die of hernias if insurance paperwork isn’t up to scratch.
But glance at other healthcare systems, and you find far more nuance. Hybrid systems that invite patient choice and drive up standards while preserving free access alongside state mandated assurances.
The pandemic has exposed the perilous position of the UK healthcare system, with its ailments clear to see, but lacking honest consultation, where diagnosis and cure may be found. Today, an almost insurmountable backlog will cost lives. Nightingale Hospitals barely opened their doors while essential outpatient departments gathered dust. Millions paid into the private sector to handle the overflow, never actually used.
We earnestly put rainbows in our window and weeped as we extolled our lifesavers. Our NHS.
But it doesn’t feel like OUR NHS to the widow whose husband didn’t get a diagnosis and is in the hospital morgue. It doesn’t feel like OUR NHS to the person refused innovative life-saving medicine who has to crowdfund to go abroad where part private healthcare offers a range of treatments a state-backed service simply cannot justify.
Whisper it quietly. Perhaps the private sector could be the saviour of the service, not its assassin. Underpaid nurses might find their wages higher and the tools needed for their job more plentiful.
While I was hobbling on crutches in Belgium three years ago, strangers crossed the street to ask me which hospital I went to. Notes are compared on clinics as casually as we chat about the weather. The hospital recommended by my GP who I could call personally, was so sought after it was building new wings packed with cutting edge technology, dinners were served under a cloche, waiting times were never more than minutes and the single room I was allocated after emergency surgery was as good as a room at the Ritz. Patient choice had driven competitive standards of care.
Yet this is a conversation we are simply not allowed to have, as minor surgery is carried out in prefab huts in car parks and it can take a whole day to get through to your GP's reception. Meanwhile some trusts are spending a sixth of their budget on repayment of private sector debts taken in the nineties to build new hospitals.
It is not just absurd, but murderous, to not be able to discuss crucial issues that measure their severity in corpses, due to a fear of speaking out.
Today, we need to talk about the NHS.